Website | E-Mail Me| Newsroom | Subscribe | Unsubscribe Website | E-Mail Me| Newsroom | Subscribe | Unsubscribe |
January
Keaveny Connection |
Contact: Stacy Morse
(573) 751-3599 |
|
Open Enrollment for Health Insurance Marketplace
Helping Patients with Severe Medical Conditions
Sen. Keaveny Files Legislation to Change Eyewitness Identification Guidelines |
Update on Medicaid
2017 Marketplace Input Needed
2015 Health Gaps Report |
| Open Enrollment for Health Insurance Marketplace |
 |
| Open enrollment for 2016 ends on January 31. |
This year, open enrollment for the 2016 health insurance marketplace ends January 31, 2016. There are several ways to learn more about the ACA or the federal Health Insurance Marketplace:
Cover Missouri: Helping Missourians Find Affordable Health Insurance
Cover Missouri is a coalition of community organizations from around Missouri that are dedicated to helping consumers understand their insurance options. Coalition members include Navigators and Certified Application Counselors (CAC), who can assist you to:
- Understand and navigate new health insurance rules and requirements;
- Understand health insurance basics;
- Research and understand ways to help pay for health insurance;
- Understand the Missouri Health Insurance Marketplace, rules and restrictions; and,
- Help understand where and how to purchase insurance.
There are no fees to use the marketplace or to receive help from a Navigator or CAC. No one should solicit health coverage to you. Here is a checklist of information you will need when you sign up:
- Social Security Number (or document numbers for legal immigrants);
- Employer and income information for every member of your household who needs coverage (for example, from pay stubs or W-2 forms—Wage and Tax Statements); and
- Policy numbers for any current health insurance plans covering members of your household.
If you are in need of a plan, you must sign up by January 31, unless your family qualifies for a Special Enrollment Period. This time-frame is a time period outside of open enrollment when you and your family have a right to sign up for health coverage. In the Marketplace, you qualify for a special enrollment period 60 days following certain life events that involve a change in family status, like marriage, the birth of a child or loss of other health coverage.
|
| Helping Patients with Severe Medical Conditions |
  |
| This is the second year legislation has been filed seeking to expand the number of medical conditions that can be treated with CBD oil in our state. |
For the 2016 legislative session I have again filed Senate Bill 822, which would expand the number of medical conditions that can be treated with Cannabidiol (CBD) oil in Missouri.Senate Bill 822 would allow people with cancer, HIV, AIDS, amyotrophic lateral sclerosis, Parkinson’s disease, multiple sclerosis, spinal cord damage, inflammatory bowel disease, neuropathies, Huntington’s disease, post-traumatic stress disorder, or certain specified symptoms or complications associated with these conditions, to have access to CBD oil. The oil must be recommended by a neurologist or physician. The Department of Health and Senior Services would be required to establish a public registry of physicians and neurologists who recommend hemp extract for the patient’s use.
CBD oil has been shown to reduce nausea and vomiting, suppress seizure activity, and combat inflammatory disorders, neurodegenerative disorders, tumor and cancer cells, and anxiety and depression disorders. Research has also shown that CBD inhibits the proliferation of cancer cells, and has found that CBD can be used to treat rheumatoid arthritis, autoimmune diseases, nausea, bowel disorders and diabetes.
It is important to remember, that unlike THC, the compound in marijuana known for its mind-altering properties, CBD oil does not produce those side effects and is not a psycho-active drug.
There are real medical benefits from CBD oil, something scientists have supported for years. Studies have shown it can be incredibly effective in lessening the severity of symptoms for a whole host of chronic conditions. Legislation has been passed out of this very body, and signed by the governor, allowing those with intractable epilepsy to use CBD extract to help treat their illness. There is no reason to only allow certain patients to benefit from what has been recognized as a legitimate form of treatment. The legislation would allow citizens suffering from cancer, Parkinson’s, and numerous other tragic diseases to have the option of using a natural substance to reduce symptoms.
This measure would require the department to issue a card to a patient who has a recommendation from a physician or neurologist stating they would benefit from treatment with hemp extract. The bill also expands the number of licensed cultivation and production facilities in the state from two to 10. |
| Sen. Keaveny Files Legislation to Change Eyewitness Identification Guidelines |
| This session I have again introduced Senate Bill 842, which will require the implementation of eyewitness identification policies that have been scientifically proven to protect against misidentification, a top contributor to wrongful conviction, proven by DNA evidence in Missouri and nationally.
There are numerous reasons to file this legislation. Missouri needs policies to safeguard against eyewitness misidentification. All nine of Missouri’s DNA exonerees were misidentified. The well-documented problems of eyewitness memory, the dangers of misidentification and the injustice that occurs when police do not implement scientifically supported eyewitness identification practices must be stopped.
Eyewitness misidentification is the leading cause of wrongful convictions in our country, contributing to 71 percent of the 336 wrongful convictions that have been proven through post-conviction DNA testing. Missouri’s nine exonerees were wrongfully convicted in part or entirely based on faulty identifications by victims and other witnesses. Those innocent men spent years of their lives in prison, while the real perpetrators were free, putting the people of Missouri in danger. New eyewitness identification policies will include, but not be limited to:
- Lineup administrator who does not know or is positioned in such a way they cannot see which lineup members are being viewed by the eyewitness: The officer conducting a live or photo lineup must not know the suspect’s identity. This prevents any unintentional cues. As it is not always practical for a small department to administer a live or photo lineup this way, the “folder shuffle” method can be alternatively used for photo lineups. This simple method involves placing photos in different folders, shuffling them and handing them to the eyewitness or victim individually, so the officer is unaware of the photo being viewed.
- Instructions: The officer must instruct the eyewitness or victim that the suspect may or may not be in the identification procedure and that the investigation will continue regardless of whether a selection is made, thus eliminating pressure to make a selection.
- Confidence statement: A verbatim statement of confidence must be written down by the officer at the time the victim or eyewitness makes an identification. Because confidence can be artificially inflated – through confirming feedback – between the time an identification is made and the case going to trial, it is important to lock in the level of initial confidence voiced by the eyewitness.
- Proper filler selection: No lineup member should stand out. Additionally, lineup members must match the victim’s or eyewitness’s description of the perpetrator.
|
| Update on Medicaid |
|
Enrollment in Medicaid has increased. However, we know there are a large number of our fellow Missourians who still need care and cannot afford the health coverage they need.
In Missouri, it is estimated that while between 250,000 and 300,000 people are eligible for Missouri’s Medicaid program, many of them do not make enough to qualify for subsidized insurance on the healthcare exchange.
There are a large number of Missourians who do not have the healthcare they need, but would be eligible for that care, should they be residents of Iowa, Illinois, Kentucky or Arkansas. The proven solution is Medicaid expansion. It is common-sense use of both federal and state legislation and funds that will save lives. Medicaid expansion is a priority of mine for the 2016 session.
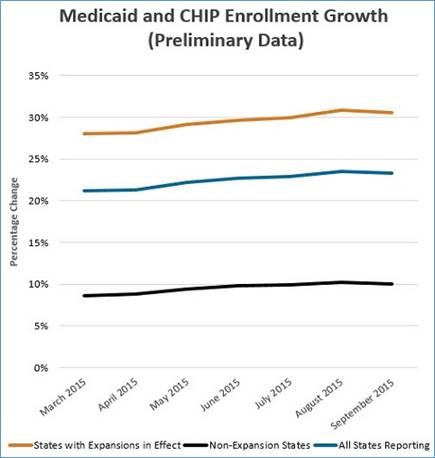
It is encouraging to see the increase in both the number of residents who are getting and receiving care. Updated information on Medicaid enrollment shows:
- Since late 2013, enrollment has increased to 13.3 million nationally;
- Enrollment is up 30 percent in states that have expanded Medicaid;
- Enrollment has only increased by 10 percent in states that have not expanded; and
- Enrollment in Medicaid in Missouri has increased by 80,000 people, or 9.5 percent.
The Centers for Medicare & Medicaid Services (CMS) released the September 2015 monthly report on state Medicaid and Children’s Health Insurance Program (CHIP) eligibility and enrollment data. These data were reported by state Medicaid and CHIP agencies as part of the Medicaid and CHIP Performance Indicator process.
The full report is available at www.Medicaid.gov or here. |
| 2017 Marketplace Input Needed |
| The Centers for Medicare & Medicaid Services (CMS) is asking for comments on proposals that will provide continued choice and competition for consumers, in a growing market for affordable healthcare plans. The proposed rule seeks to improve the consumer experience, both when individuals shop for health insurance and when they use it.
The Health Insurance Marketplace continues to grow as we enter the third year. It is estimated that tens of thousands of Americans will need, and turn to, marketplace plans.
In an effort to ensure fewer people face surprises after buying a policy, CMS is seeking comment on a requirement that health plans in the federal Marketplace count certain out-of-pocket expenses on unexpected out-of-network services. If a patient who had surgery at an in-network facility finds out later that their anesthesiologist, for example, was not part of the health plan’s network, cost-sharing charges for that anesthesiologist’s services would count toward the out-of-pocket maximum. Currently, these types of out-of-network cost-sharing charges are usually not counted towards the out-of-pocket maximum.
Recognizing that once consumers enroll in coverage, many still need assistance in understanding and using their coverage, the proposed rule seeks comment on expanding the required duties of navigators. Expanded duties would include certain post-enrollment assistance like Marketplace eligibility appeals, applying for exemptions through the Marketplace, and navigating from coverage to care. This proposal is a step forward in engaging and empowering consumers with the resources they need to understand how to use their coverage.
The proposed rule would also increase options for employees in the federal Small Business Health Options Program (SHOP) for plan years beginning in 2017. Under current regulations, employers participating in the federal SHOP Marketplace can offer their employees either one health plan and/or one dental plan, or all health and dental plans across one level. Under the proposal, employers would be able to offer all plans across all levels of coverage from one insurance company. This would give employers more choices as they look for coverage that best fits their employees.
The rule proposes changes and asks for comments on several proposals as well as improvements to the premium stabilization programs in an ongoing effort to build the Marketplace. Those include:
- Streamlining enrollment so customers can more easily use websites of agents and brokers, decreasing administrative costs;
- Keeping the federal Marketplace user fee the same for 2017;
- Discussing options for transitioning consumers smoothly from Marketplace coverage to Medicare, so that elderly move from the Marketplace risk pool to Medicare;
- Recalibrating the risk adjustment formula using most recent data to provide greater accuracy of payments;
- Requesting comments on improvements to the child age rating to reflect risk more accurately, so premiums can be more accurately priced; and
- Seeking comment on the Open Enrollment period for 2018 and beyond.
Details of the Public Comment Period:
- The public is encouraged to submit general comments relevant to both measures or comments specific to certain measures;
- Do not include personal health information in your comments; and
- At the end of the public comment period, all public comments will be posted on the website along with a public comment summary report
Instructions for Providing Comments:
- If you are providing comments on behalf of an organization, include the organization’s name and your contact information;
- If you are commenting as an individual, submit identifying or contact information;
- Please indicate which measure(s) you are commenting on; and
- You may submit general comments on the entire set of measures or you may provide comments specific to individual measures.
|
| 2015 Health Gaps Report |
|
|
| In Missouri, while it is estimated between 250,000 and 300,000 mostly working people are eligible for Missouri’s Medicaid program, many of them do not make enough to qualify for subsidized insurance on the healthcare exchange. |
|
|
A recent study released by the St. Louis Regional Health Commission (RHC) shows emergency room visits in the St. Louis area are down about 5 percent from previous years. The decrease in visits is tied to the increased number of St. Louis residents who have health insurance through the healthcare exchange. However, the number of visits could decrease even more, if the state would expand Medicaid.
There were about 7,000 fewer emergency room visits to St. Louis area hospitals in 2014. Some of the decrease is due to the number of residents who have health insurance that once did not. However, there are also a large number of people who have high-deductible plans and simply cannot afford to go to the emergency room. While there are 23,300 more St. Louis area residents with health insurance than there were in 2010, many are still uninsured or under-insured. We still have friends and neighbors who need access to healthcare.
The new Missouri’s Health Gaps Report found 3,800 premature deaths in Missouri could be prevented each year if significant gaps in opportunities for good health among Missouri’s counties were eliminated. The report—released by the Robert Wood Johnson Foundation and the University of Wisconsin Population Health Institute—details how well the healthiest counties do; demonstrates the difference that could be made if every county had the same chance to be healthy; and provides strategies to close the gaps between the healthiest and least healthy places. |
 |
|
|